

Giving Doctors Their Time Back: An Ambient AI Medical Scribe
High-level overview of a zero-to-one product I led as CTO. No patient data, model weights, or proprietary details are disclosed.
The business problem
Ask any physician what they like least about their job and the answer is rarely the medicine — it’s the documentation. For every hour of patient care, clinicians spend roughly another hour on notes, much of it after the last patient goes home. The industry has a name for it: pajama time. It is a leading driver of burnout, it shortens the time a doctor can actually look at a patient, and it quietly caps how many patients a practice can see.
The opportunity is simple to state and hard to build: the richest source of a clinical note is the conversation that already happens in the room. If software could listen to the visit and draft the note — HPI, physical exam, assessment, plan — and suggest the billing codes, the physician’s job would shrink from writing to reviewing.
That was the product I led, from concept to a pilot across 50+ physicians, as CTO of a seed-funded startup: an ambient AI medical scribe — internally, the project that gives doctors their time back.
What it does
- Listen — with consent, the app captures the ambient audio of the patient–provider conversation on the clinician’s phone.
- Transcribe — speech-to-text turns the conversation into an accurate, speaker-aware transcript.
- Draft — language models tuned for clinical language turn that transcript into a structured note (History of Present Illness, Physical Exam, Assessment & Plan) and suggest ICD-10 diagnosis and CPT procedure codes for billing.
- Review & sign — the physician reviews and edits the draft and signs off. The AI never has the last word; it produces a first draft a clinician approves.
The design principle throughout: the model does the typing, the clinician keeps the judgment.
Architecture overview
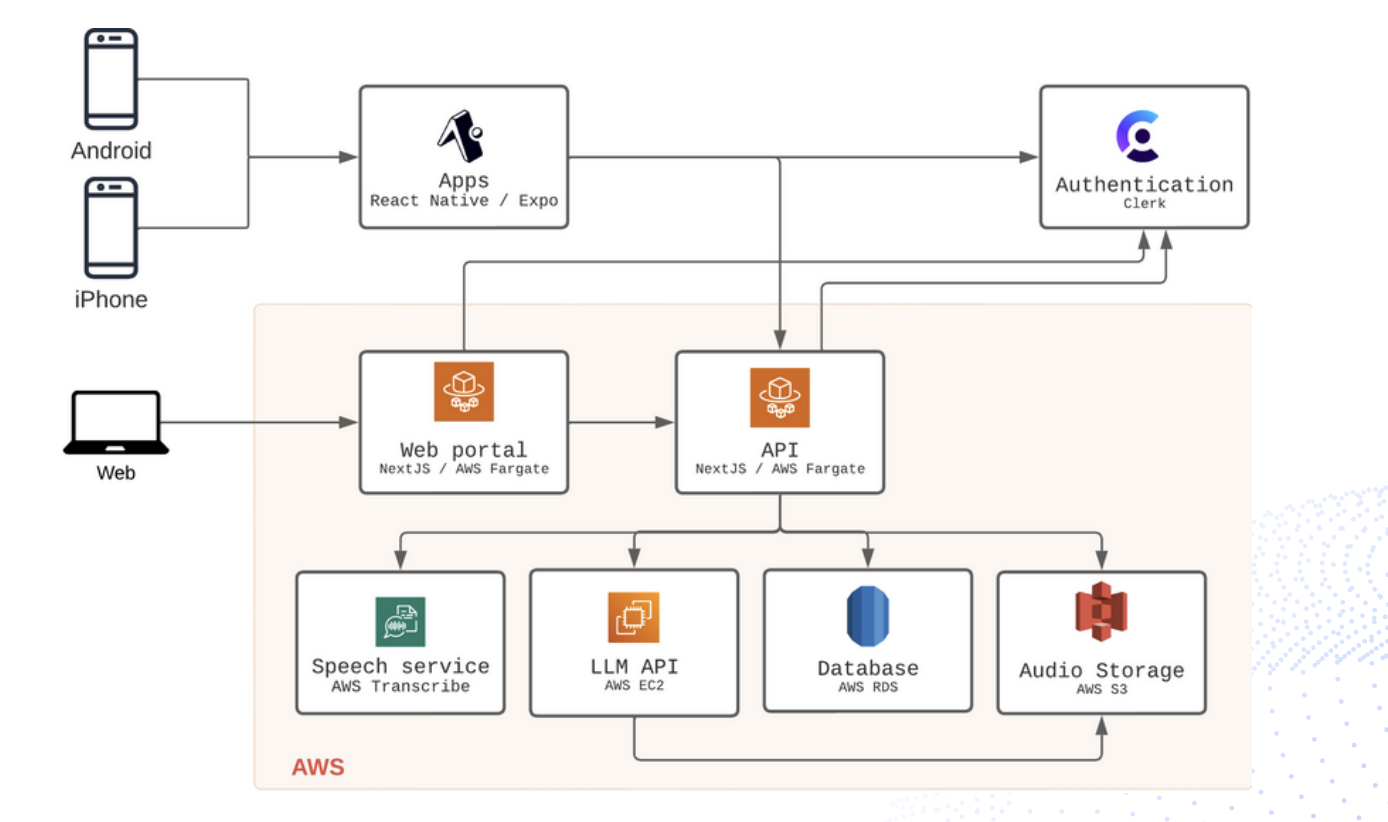
A mobile-first product on a cloud backend:
- Clients — native iOS and Android apps (React Native / Expo) for capture in the exam room, plus a web portal for review and administration.
- Authentication — a managed identity provider handles sign-in and session security so we never build or store credentials ourselves.
- API & web tier — containerized services on managed compute host the application and the review portal.
- Speech service — a managed speech-to-text service produces the transcript from captured audio.
- LLM service — the clinical language models that generate the note and code suggestions run behind our own inference API, so we control prompts, models, and safety behavior.
- Data & storage — a managed relational database holds structured clinical and account data; object storage holds the audio artifacts.
Under the hood, the note-generation models were adapted from the clinical NLP literature — approaches like medical-domain language models and instruction-tuned clinical summarizers — and paired with structured ICD-10 / CPT reference data so code suggestions map to real, billable codes rather than plausible-sounding text.
In the exam room Cloud backend Physician
┌───────────────┐ audio ┌──────────────┐ transcript ┌───────────────┐
│ mobile app │──────────▶ │ speech-to- │─────────────▶ │ clinical LLM │
│ (ambient │ │ text │ │ → HPI, exam, │
│ capture, │ └──────────────┘ │ A&P + ICD-10│
│ with consent)│ │ / CPT codes │
└───────────────┘ └──────┬────────┘
│ draft note
┌───────▼────────┐
│ human-in-the- │
│ loop review & │
│ sign-off │
└────────────────┘
What was hard (and interesting)
- Clinical language is its own dialect. General-purpose transcription and summarization stumble on medication names, abbreviations, and the implicit structure of a clinical encounter. Domain-adapted models and careful prompt design moved the needle far more than raw model size.
- Coding has to be correct, not merely fluent. A confident but wrong ICD-10 or CPT suggestion is worse than none. Grounding suggestions in the actual code sets — and keeping a human in the loop — was essential.
- Trust is the product. Physicians will adopt a scribe that saves them time only if the draft is good enough that reviewing it is faster than writing from scratch. Every design decision came back to that bar.
- Zero-to-one and a distributed team. I built and led a geographically distributed team of ML engineers, software engineers, and product managers, taking the product from an idea to something running in real clinics.
Takeaways
- The best data is the conversation you’re already having. Ambient capture turns documentation from a writing task into a reviewing task.
- Domain beats scale for clinical NLP — adapting models to medical language and grounding codes in real reference data mattered more than model size.
- Human-in-the-loop isn’t a constraint, it’s what makes it adoptable in a setting where errors have real consequences.
- Measure adoption by time saved. If reviewing the draft isn’t clearly faster than writing the note, nothing else about the technology matters.